
Rhonda Cole has worked for ETSU Physicians for 34 years. Hard to imagine, huh? And for most our pre-EHR employees, when the computer programs screwed up, bit the dust, or became inoperable by some other clichéd demise, Rhonda was a phone call away. She still is the go-to for many of our practice management computer programs, but with the implementation of the Allscripts EHR, a whole new team, with a dedicated line just for EHR issues, was formed.
Now, when someone has computer problems, they usually aren’t singing “Help Me, Rhonda,” more like “Help, I Need Somebody … who will help me with this #?!*&%^ EHR.” It’s not that they prefer the Beatles over The Beach Boys, or that they don’t like talking to Rhonda. It’s just the tune we have to play now. Rhonda’s computer program issues may be a nuisance to many that have to call her, but most of the issues don't keep providers from seeing patients. More often than not, though, when someone calls the EHR Helpdesk, they can’t continue to work because they are frozen or have received an error message. Without access to the chart, they feel powerless to help the patient.
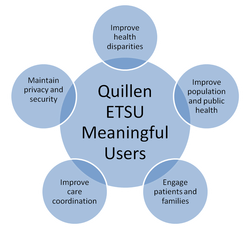
So, I probably just validated all of the negative thoughts you’ve been having about using an EHR, but what about the positive aspects of the system? What makes it better than all that paper? What makes it meaningful?
For a while, Rhonda was one of the few people who could pull data for ETSU. She was the person to see for reports on codes and charges, or else, clinic personnel would have to take the time to manually pull data—a very time consuming and expensive task. Now, a call or task to the EHR Helpdesk can provide users with meaningful data that we could never easily gather before. For instance, we regularly run reports on Controlled Drugs that are prescribed in some of our clinics for quality assurance. We are also currently generating a report on patients with HIV and CAD for providers heading up a research study. We can also generate patient lists by request for providers wanting to keep track of a specific patient demographic or diagnosis.
Now, when someone has computer problems, they usually aren’t singing “Help Me, Rhonda,” more like “Help, I Need Somebody … who will help me with this #?!*&%^ EHR.” It’s not that they prefer the Beatles over The Beach Boys, or that they don’t like talking to Rhonda. It’s just the tune we have to play now. Rhonda’s computer program issues may be a nuisance to many that have to call her, but most of the issues don't keep providers from seeing patients. More often than not, though, when someone calls the EHR Helpdesk, they can’t continue to work because they are frozen or have received an error message. Without access to the chart, they feel powerless to help the patient.
So, I probably just validated all of the negative thoughts you’ve been having about using an EHR, but what about the positive aspects of the system? What makes it better than all that paper? What makes it meaningful?
For a while, Rhonda was one of the few people who could pull data for ETSU. She was the person to see for reports on codes and charges, or else, clinic personnel would have to take the time to manually pull data—a very time consuming and expensive task. Now, a call or task to the EHR Helpdesk can provide users with meaningful data that we could never easily gather before. For instance, we regularly run reports on Controlled Drugs that are prescribed in some of our clinics for quality assurance. We are also currently generating a report on patients with HIV and CAD for providers heading up a research study. We can also generate patient lists by request for providers wanting to keep track of a specific patient demographic or diagnosis.

There is also the convenience to the patient of providers being able to send prescriptions electronically so that the medications are waiting at the pharmacy, or the quick access to last week’s or last month’s or last year’s labs.
The patient’s accessibility to results and medical data is also greatly improved. As they leave the clinic, a clinical summary is easily generated if desired, and very soon, an electronic portal will be available to the patient.
And what about provider accessibility? The patient’s record is now accessible from home, from the hospital, even from a smart phone. That kind of convenient accessibility has never been a option—on-call providers had to fly blind.
Obviously, EHR isn’t perfect and probably never will be. Ask Rhonda. She’s been working with computers and software that still need buggy problems fixed. She’s heard the song before: “And I can give you lotsa reasons why/ You gotta help me, Rhonda.” (The Beach Boys, Help Me, Rhonda)
But since we have a new program, and a new team, a new number to dial, how about we try singing a new song:
“(Now) But now these days are gone (These days are gone), I'm not so self assured/
(I know I've found) Now I find I've changed my mind and opened up the doors.” (The Beatles, “Help!”)
The patient’s accessibility to results and medical data is also greatly improved. As they leave the clinic, a clinical summary is easily generated if desired, and very soon, an electronic portal will be available to the patient.
And what about provider accessibility? The patient’s record is now accessible from home, from the hospital, even from a smart phone. That kind of convenient accessibility has never been a option—on-call providers had to fly blind.
Obviously, EHR isn’t perfect and probably never will be. Ask Rhonda. She’s been working with computers and software that still need buggy problems fixed. She’s heard the song before: “And I can give you lotsa reasons why/ You gotta help me, Rhonda.” (The Beach Boys, Help Me, Rhonda)
But since we have a new program, and a new team, a new number to dial, how about we try singing a new song:
“(Now) But now these days are gone (These days are gone), I'm not so self assured/
(I know I've found) Now I find I've changed my mind and opened up the doors.” (The Beatles, “Help!”)










 RSS Feed
RSS Feed